Drug-Induced Pulmonary Fibrosis Risk Checker
This tool assesses your potential risk of developing drug-induced pulmonary fibrosis based on medications you're taking and symptoms. Remember: most people taking these medications never develop lung damage, but early detection is crucial.
Medication Information
Symptom Check
Select any symptoms you're experiencing:
Results will appear here after assessment
What Is Drug-Induced Pulmonary Fibrosis?
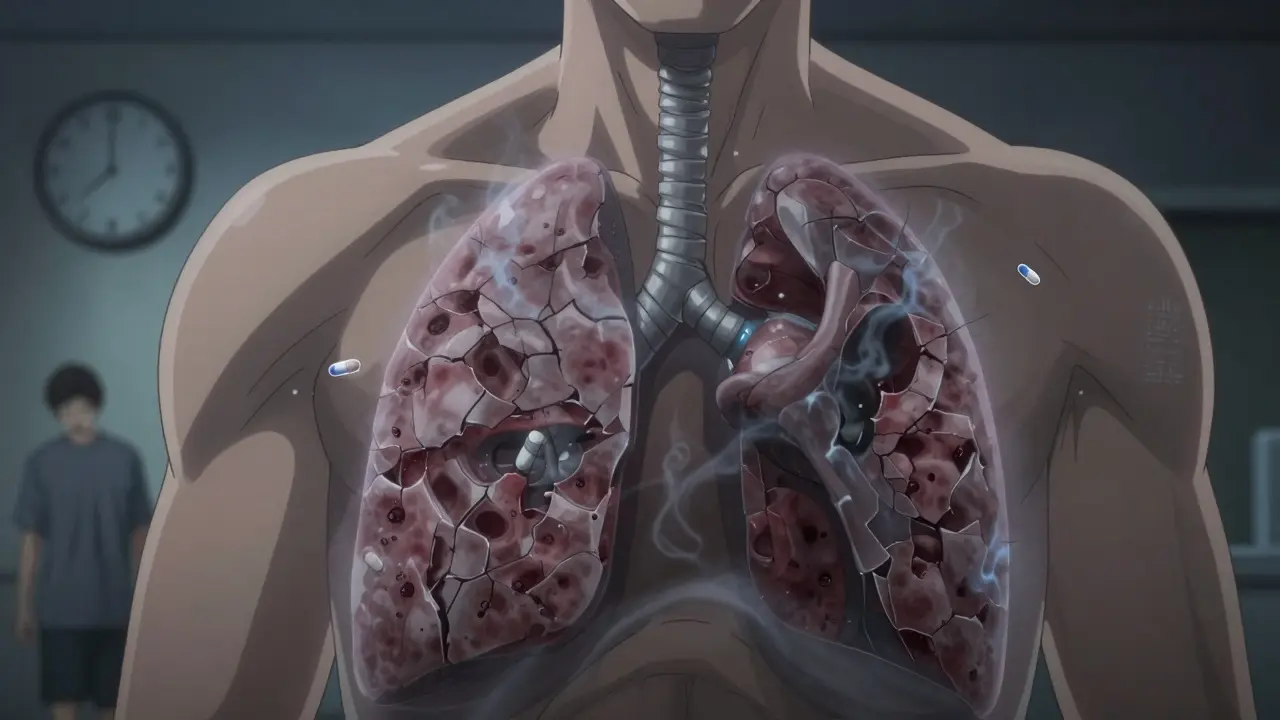
Most people don’t think about their lungs when taking a pill for a urinary infection, arthritis, or cancer. But some medications quietly scar the lungs over time - not with a sudden crash, but with a slow, creeping damage called drug-induced pulmonary fibrosis (DIPF). It’s not common, but when it happens, it’s serious. Your lungs fill with stiff, fibrous tissue instead of soft, stretchy air sacs. Breathing becomes harder. A dry cough sticks around. You get tired just walking to the kitchen.
This isn’t asthma or pneumonia. It’s scarring - permanent damage that doesn’t heal easily. And it’s not caused by smoking or pollution. It’s caused by drugs you’re supposed to trust. The worst part? You might not notice it until it’s too late. Symptoms often look like aging, getting out of shape, or a lingering cold. By the time doctors catch it, the damage is already done.
Which Medications Are the Biggest Culprits?
Over 50 medications have been linked to lung scarring. But a few stand out as the most dangerous. According to data from New Zealand’s pharmacovigilance system (2014-2024), three drugs account for nearly half of all reported cases:
- Nitrofurantoin - Used for urinary tract infections, especially in older adults taking it long-term to prevent flare-ups. Symptoms can show up after 6 months or even 10 years.
- Methotrexate - Commonly prescribed for rheumatoid arthritis and psoriasis. It can trigger sudden lung inflammation that turns into scarring within weeks.
- Amiodarone - A heart rhythm drug taken for years. After a cumulative dose over 400 grams (usually 6-12 months of use), it starts damaging lung tissue in 5-7% of patients.
Then there are the cancer drugs. Bleomycin, used in chemotherapy for lymphoma and testicular cancer, causes lung damage in up to 20% of patients. Cyclophosphamide and methotrexate (also used in cancer) add to the risk. Even newer immunotherapy drugs - like pembrolizumab and nivolumab - are now being linked to this condition. These are supposed to boost your immune system to fight cancer. But sometimes, they turn it against your lungs.
Why Do Only Some People Get It?
If these drugs are so dangerous, why don’t everyone who takes them end up with scarred lungs? The answer is simple: we don’t fully know. It’s not about the dose. It’s not about how long you’ve been on the drug. Two people can take the same pill, same dose, same length of time - one stays healthy, the other develops life-threatening lung scarring.
Researchers believe genetics play a role. Some people’s bodies process these drugs in a way that creates toxic byproducts that attack lung cells. Others have immune systems that overreact, mistaking lung tissue for a threat. Age matters too - most cases happen in people over 60. But even younger patients aren’t safe. There’s no blood test to predict who’s at risk. No scan can spot it before damage begins. That’s why early symptoms are your only warning.
What Are the Early Warning Signs?
These symptoms creep in slowly. People often ignore them. They think, “I’m just getting older,” or “I’m not as fit as I used to be.” But if you’re on one of these high-risk drugs, don’t brush them off:
- A dry cough that won’t go away - no mucus, no fever, just constant irritation
- Shortness of breath during light activity - climbing stairs, carrying groceries, talking while walking
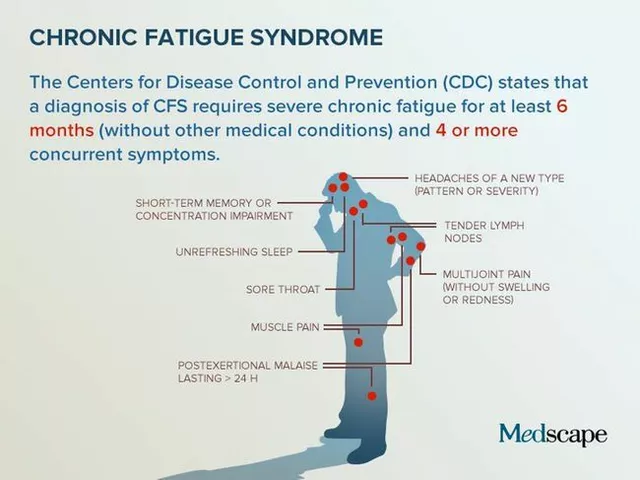
- Unexplained fatigue - feeling wiped out even after a full night’s sleep
- Chest discomfort or aching - not like a heart attack, but a dull, persistent tightness
- Fever or joint pain - less common, but sometimes the body’s immune system is in overdrive
One patient from a pulmonary fibrosis support group described it: “I thought I was just winded from walking the dog. Turns out, my lungs were filling with scar tissue. I didn’t know until I collapsed in the grocery store.”
Studies show the average delay between first symptoms and correct diagnosis is over eight weeks. That’s eight weeks of ongoing damage. The longer you wait, the less likely your lungs can recover.
How Is It Diagnosed?
There’s no single test for drug-induced pulmonary fibrosis. Doctors have to rule everything else out. That means:
- A detailed medication history - every pill you’ve taken in the last year, even over-the-counter ones
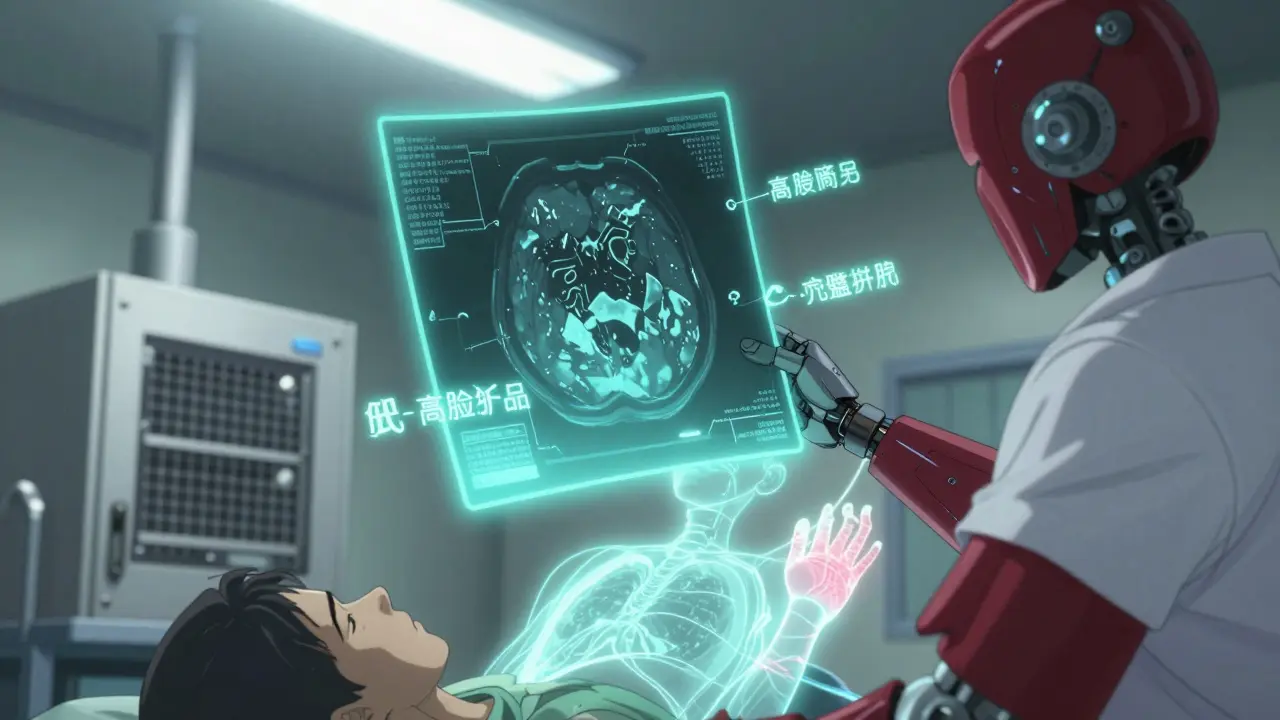
- A high-resolution CT scan of your chest - this shows the pattern of scarring in the lungs
- Pulmonary function tests - measures how well your lungs move air and transfer oxygen
- Blood tests - to check for signs of inflammation or autoimmune activity
- Possible lung biopsy - if the diagnosis is still unclear, a small tissue sample may be taken
The tricky part? The scarring looks the same whether it’s caused by a drug, asbestos, or an unknown autoimmune disease. That’s why your medication history is the most important clue. If you’re on amiodarone and your CT scan shows patchy scarring, your doctor should suspect drug-induced fibrosis - not assume it’s just aging.
Can It Be Reversed?
Yes - if caught early. The first and most critical step is stopping the drug. In 89% of cases, lung damage stops progressing once the medication is discontinued. Many patients start feeling better within three months. Some even regain most of their lung function.
But if the scarring is advanced, recovery is limited. About 15-25% of patients end up with permanent damage. That’s why timing matters. The sooner you act, the better your chances.
Treatment usually includes:
- High-dose steroids - Prednisone is often prescribed for 3-6 months to calm inflammation and slow scarring
- Oxygen therapy - If your blood oxygen drops below 88%, you may need supplemental oxygen at rest or during activity
- Pulmonary rehab - Breathing exercises, light exercise training, and education to help you manage symptoms
There are no drugs that reverse fibrosis yet. But research is underway. Scientists are testing genetic markers to predict who’s at risk before they even start the medication. One day, a simple blood test might tell you if you’re vulnerable to amiodarone or methotrexate before you take the first pill.

What Should You Do If You’re on One of These Drugs?
You don’t need to panic. Most people who take these medications never develop lung damage. But you should be informed. Here’s what to do:
- Know your risk - If you’re on nitrofurantoin, amiodarone, methotrexate, or any cancer immunotherapy, ask your doctor if you’re at risk for lung damage.
- Get baseline lung tests - Before starting high-risk drugs, ask for a pulmonary function test and a chest X-ray. Keep a copy.
- Watch for symptoms - If you develop a dry cough or shortness of breath, don’t wait. See your doctor immediately.
- Don’t stop medication on your own - Stopping a heart or cancer drug without medical guidance can be dangerous. Talk to your doctor first.
- Ask about alternatives - Is there another antibiotic that won’t harm your lungs? Is there a different arthritis drug that doesn’t carry this risk?
Doctors are getting better at this. In clinics that screen patients on high-risk drugs, diagnostic delays have dropped by 32%. But many primary care providers still don’t ask about breathing problems when prescribing these meds. You have to be your own advocate.
The Bigger Picture
Drug-induced pulmonary fibrosis is rising. Reported cases have jumped 23.7% over the last decade. Why? More people are taking these drugs. More drugs are being developed. And we’re finally starting to recognize the pattern.
Regulatory agencies like Medsafe in New Zealand and the FDA are now requiring stronger warnings on labels. In 2024, New Zealand’s medicines committee specifically told doctors to remind patients about lung risks before prescribing methotrexate or amiodarone.
But the real solution isn’t just better warnings. It’s better screening. It’s routine lung tests before starting risky drugs. It’s research into genetic risk factors. And it’s giving patients the tools to speak up - before their lungs turn to stone.
Final Thought
Medicines save lives. But they can also harm in ways we don’t always see. Drug-induced pulmonary fibrosis is silent, slow, and often missed. If you’re taking a long-term medication - especially for heart, lung, joint, or cancer conditions - pay attention to your breathing. Don’t assume it’s just age. Don’t wait for a cough to go away. Talk to your doctor. Get tested. Your lungs can’t tell you they’re hurting. You have to speak for them.

12 Comments
Alec Stewart Stewart
This hit me hard. My grandma was on nitrofurantoin for years and no one ever told her about lung risks. She just kept saying she was "getting winded." 😔 Now she’s on oxygen. Please, if you’re on any long-term med, ask your doc about this. Your lungs can’t scream for help.
Demetria Morris
People treat medicine like candy. You pop a pill like it’s a gummy bear and expect zero consequences. This is why we have a healthcare crisis-because no one takes responsibility for their own body anymore.
Geri Rogers
Y’ALL. This is SO IMPORTANT. 🙌 I’m a nurse and I’ve seen this happen 3x in the last year. Amiodarone is a silent killer. If you’re on it, get a baseline PFT. Do it. Don’t wait till you’re gasping at the grocery store. Your doctor might not know-so YOU have to push. 💪❤️
Caleb Sutton
Big Pharma knows this. They’ve known for decades. They just don’t care. They’re making billions off your broken lungs. The FDA? A puppet. The system is designed to kill quietly. You’re not sick-you’re being harvested.
Jamillah Rodriguez
I read this and thought… cool, but I’m not on any of those meds. Then I remembered I took methotrexate for 8 months for my psoriasis. 🤔 Should I be worried? Idk. Maybe I’ll Google it later.
Susheel Sharma
The systemic negligence exhibited in pharmacovigilance protocols is nothing short of grotesque. One cannot help but observe the commodification of human physiology in the context of polypharmaceutical regimes. The absence of mandatory pulmonary screening constitutes a structural failure of bioethical governance.
Janice Williams
This is why I stopped trusting doctors. They prescribe like they’re playing Russian roulette with your organs. And now you’re supposed to be grateful they didn’t kill you faster? Pathetic.
Roshan Gudhe
There’s a deeper truth here: we’ve outsourced our bodily wisdom to pills. We forget that the body is not a machine to be fixed, but a living system that whispers before it screams. These drugs don’t just scar lungs-they silence intuition. Maybe the real question isn’t which drug harms, but why we stopped listening to ourselves.
Rachel Kipps
i didnt know this could happen... i take amiodarone and i've had a dry cough for months. i thought it was just allergies. should i go to the dr? i'm scared.
Wendy Lamb
My dad’s on methotrexate. I’m printing this out and handing it to his rheumatologist tomorrow. Thanks for sharing.
Amit Jain
In India, we don’t even get proper warnings. My aunt took nitrofurantoin for 5 years. No one told her. She got diagnosed when she couldn’t walk to the bathroom. Don’t wait. Get tested.
rahulkumar maurya
You people are so naive. This isn’t about medication-it’s about the decay of Western medicine. We’ve replaced wisdom with algorithms. A 65-year-old woman on amiodarone? She should’ve been on a plant-based diet and yoga. But no, we’d rather poison her and call it science.