Pharmacogenomics Risk Calculator
This calculator estimates your risk of adverse drug reactions based on factors discussed in the article. Enter your information to see how your age, medications, and genetic factors could affect your drug response.
Have you ever taken the same medication as someone else - maybe a friend or family member - and had completely different results? One person feels fine, while the other ends up in the hospital with nausea, dizziness, or worse? It’s not just bad luck. It’s biology. And it’s more common than you think.
Why Your Body Reacts Differently to Pills
Medications don’t work the same way for everyone. A drug that helps one person might do nothing for another - or even make them sicker. This isn’t random. It’s rooted in how your body handles chemicals. Two key systems control this: pharmacokinetics (what your body does to the drug) and pharmacodynamics (what the drug does to your body). Your liver, kidneys, and gut decide how fast a drug gets broken down and flushed out. Your brain, heart, and other organs decide how strongly the drug affects you. And here’s the catch: these systems vary wildly from person to person. Two people taking the same dose of blood thinner might end up with wildly different blood levels - one perfectly safe, the other bleeding internally.Genes Are the Hidden Players
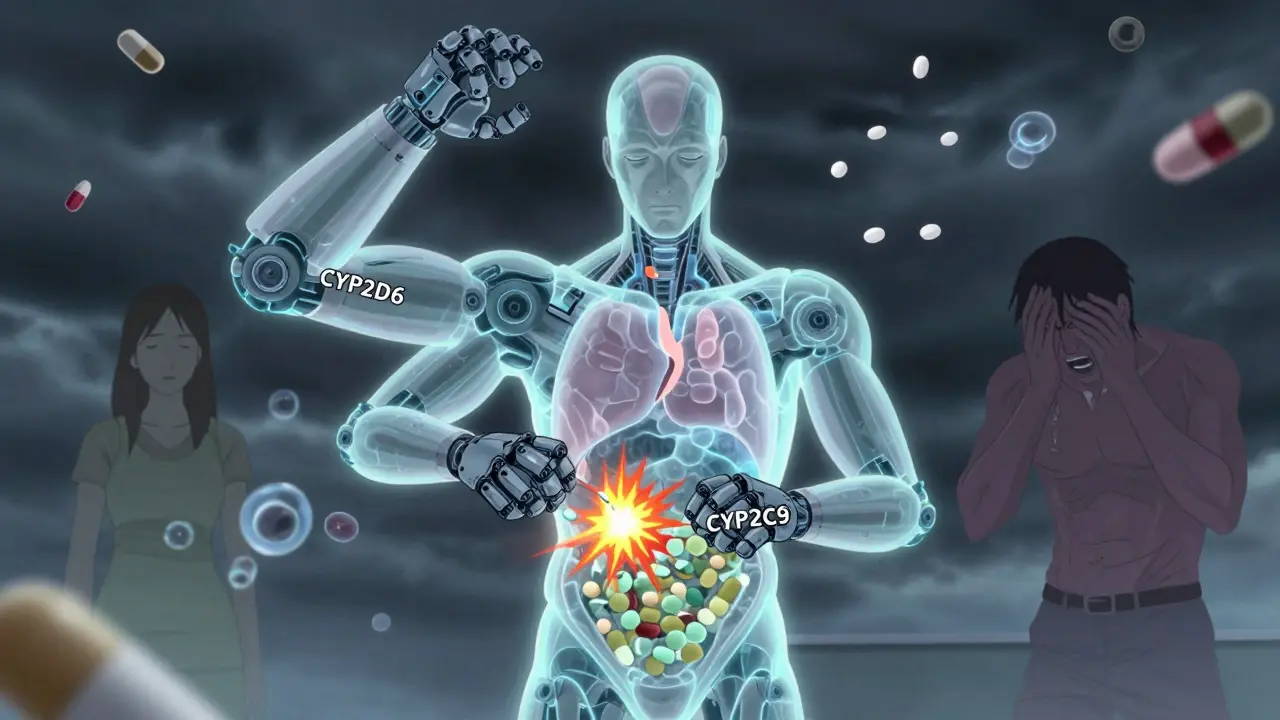
Your DNA plays a bigger role in drug response than most doctors admit. About 20% to 95% of how you react to a medication comes down to your genes. The biggest culprits? Enzymes in your liver - especially the CYP450 family. These are your body’s chemical scissors, cutting drugs into pieces so they can be removed. For example, CYP2D6 processes about 25% of all prescription drugs, including antidepressants, beta-blockers, and painkillers like codeine. About 5-10% of white people are “poor metabolizers” - their CYP2D6 enzyme barely works. They take a standard dose of codeine and get almost no pain relief because their body can’t turn it into morphine. Meanwhile, “ultra-rapid metabolizers” - common in Ethiopia and parts of North Africa - turn codeine into morphine so fast they risk overdose on normal doses. Another example: clopidogrel (Plavix), a common heart drug. About 2-15% of people have a genetic variant that makes their body unable to activate the drug. They take it, think they’re protected from heart attacks, but their blood still clots. That’s why some patients have heart attacks even while on “preventive” meds.Age, Weight, and Body Chemistry
Genes aren’t the whole story. Your age, weight, and overall health matter too. Older adults have more body fat and less muscle. Fat-soluble drugs like diazepam or antidepressants stick around longer, building up to toxic levels. A 70-year-old might need half the dose of a 30-year-old for the same drug. Kidney function drops with age. If your kidneys can’t clear a drug like metformin or lisinopril, it lingers - increasing side effects like dizziness, low blood pressure, or even kidney damage. Many elderly patients are prescribed multiple drugs without adjusting doses for declining organ function. Even something as simple as your gut bacteria can change how a drug works. Some bacteria break down drugs before they’re absorbed. Others activate them. And antibiotics can wipe out those helpful microbes - changing how you respond to future meds.Drug Interactions Are a Silent Killer
Taking more than one medication? You’re playing Russian roulette with your body. A common example: warfarin (Coumadin), a blood thinner. If you’re also taking amiodarone (for heart rhythm), your warfarin levels can spike by 100-300%. That’s not a small bump - that’s a life-threatening risk of internal bleeding. Even over-the-counter stuff can be dangerous. Ibuprofen and aspirin can interfere with blood pressure meds. St. John’s wort - a popular herbal remedy for depression - can make birth control, HIV drugs, and transplant medications useless. These aren’t rare cases. They happen daily. And it gets worse when inflammation is involved. If you have an infection, arthritis, or even a bad cold, your liver enzymes slow down by 20-50%. That means drugs build up faster than expected. A dose that was safe last week might be dangerous now.Pharmacogenomics: The Future of Personalized Medicine
There’s a growing field called pharmacogenomics - using your genes to pick the right drug and dose. It’s not science fiction. The FDA has added pharmacogenomic info to over 300 drug labels. For warfarin, testing for CYP2C9 and VKORC1 genes can cut bleeding risks by 31% and get patients to the right dose 27% faster. In pediatric cancer, testing for TPMT gene variants before giving mercaptopurine reduced severe toxicity from 25% to 12%. That’s life-saving. In asthma, patients with a specific LTC4 synthase variant respond 45% better to leukotriene blockers like montelukast - while others get no benefit at all. Imagine spending $300 a month on a drug that does nothing for you. But here’s the problem: most doctors don’t test. Only 18% of U.S. insurers cover pharmacogenomic tests. Only 32% of hospitals have systems that alert doctors when a patient’s genes conflict with a prescribed drug. And 68% of physicians say they don’t feel trained to use the results.
Why Isn’t Everyone Getting Tested?
Cost used to be a barrier. A full gene panel cost $2,000 in 2015. Now? It’s under $250. Medicare started covering tests for 17 high-risk drugs in January 2024. So money isn’t the main issue anymore. The real hurdles are system-wide. Electronic health records rarely include genetic data. Doctors don’t know how to interpret reports. Pharmacies don’t flag dangerous combinations. And there’s no standard way to share results across providers. Also, genetics isn’t perfect. Testing just CYP2D6, CYP2C9, and CYP2C19 explains only 15-19% of side effects. Hundreds of other genes are involved - and we’re still mapping them. A single-gene test won’t catch everything. That’s why some experts say we need polygenic risk scores - combining dozens or hundreds of small genetic signals to predict response.What You Can Do Right Now
You don’t need to wait for your doctor to order a test. Here’s what you can do today:- Keep a full drug list - including vitamins, supplements, and OTC meds. Bring it to every appointment.
- Ask: “Could this interact with my other meds?” Don’t assume your doctor knows everything you’re taking.
- Track side effects - write down when you feel dizzy, nauseous, or fatigued after starting a new drug. Share this with your provider.
- Ask about pharmacogenomic testing - especially if you’ve had bad reactions before, or if you’re on multiple drugs. It’s worth asking.
- Don’t ignore genetic test results - if you’ve had a test done (like through 23andMe or a clinic), share the report. Many people don’t realize these results can be medically useful.
The Bottom Line
Your body isn’t broken if a drug doesn’t work for you. It’s just different. And that’s normal. The old model - one size fits all - is outdated. We’re moving toward personalized medicine, where your genes, age, lifestyle, and other meds shape your treatment plan. The good news? We’re getting better at predicting who will react badly. The bad news? The system hasn’t caught up yet. But you can be ahead of the curve. Ask questions. Track your reactions. Push for better care. Because your body deserves more than a guess.Why do some people have side effects from drugs while others don’t?
It’s due to differences in genetics, age, weight, organ function, other medications, and even gut bacteria. For example, some people have gene variants that make them slow metabolizers - meaning drugs build up to toxic levels. Others are ultra-rapid metabolizers, so the drug gets cleared too fast to work. Even something like a cold can slow liver function and change how a drug acts.
Is pharmacogenomic testing worth it?
For people on multiple medications, those with a history of bad reactions, or those taking high-risk drugs like warfarin, clopidogrel, or certain antidepressants - yes. Testing can prevent dangerous side effects, reduce hospital visits, and save money long-term. Studies show it cuts emergency room visits by 32% and shortens hospital stays by 26%. Costs have dropped to under $250, and Medicare now covers testing for 17 key drugs.
Can I get my genes tested without a doctor’s order?
Yes - companies like 23andMe and Ancestry offer raw genetic data. But interpreting it for drug response requires medical expertise. You can upload your raw data to services like GeneSight or LifeKit, which analyze it for pharmacogenomic risks. Still, always share results with your doctor. They can confirm if the findings apply to your specific meds and health situation.
Which drugs have the strongest genetic links to side effects?
Warfarin (blood thinner), clopidogrel (antiplatelet), statins (cholesterol drugs), certain antidepressants like SSRIs, codeine (painkiller), and chemotherapy drugs like mercaptopurine. For each, specific gene variants can make the drug ineffective or dangerous. The FDA lists 44 drugs with clear genetic dosing guidelines.
Do side effects get worse as you get older?
Yes. As you age, your liver and kidneys process drugs more slowly. You also have more body fat, which holds onto fat-soluble drugs longer. Older adults are 300% more likely to have a drug reaction if they take five or more medications. That’s why polypharmacy is one of the biggest risks for seniors.


8 Comments
Carlos Narvaez
Let’s be real - if you’re still on a one-size-fits-all prescription model, you’re practicing 1980s medicine. Pharmacogenomics isn’t niche anymore. It’s basic science. The fact that insurers won’t cover it is a moral failure, not an economic one.
My cousin took Plavix for years. Had a stroke. Turns out she was a non-responder. No one tested her. No one cared. Now she’s on ticagrelor. Alive. And we’re all wondering why this isn’t standard.
It’s not about cost. It’s about laziness disguised as tradition.
Michael Dillon
Everyone’s acting like this is some revolutionary breakthrough. Newsflash: doctors have known for decades that people react differently. My grandfather took warfarin for 20 years without a single test. Lived to 92. Meanwhile, we’re overcomplicating everything with gene panels and apps.
Maybe the real problem isn’t genetics - it’s that we’ve turned medicine into a tech startup.
Harbans Singh
This is such an important post. I’ve seen this in my family - my aunt took the same antidepressant as my cousin, and one got better, the other got worse. We assumed it was ‘mental’ until we found out about CYP2D6.
As someone from India, I’ve noticed how often Western dosing guidelines don’t fit our population. Smaller body frames, different gut flora, different diets - it all matters. We need more global data, not just studies on white populations.
Also, gut bacteria? Wild. I read a study where probiotics changed how someone metabolized metformin. Who knew yogurt could be a drug interaction?
Let’s stop blaming patients for ‘not responding.’ Start testing. Start listening. It’s not magic - it’s biology.
Katherine Blumhardt
OMG I JUST FOUND OUT I’M A CYP2D6 ULTRA-RAPID METABOLIZER 😱
So that’s why codeine did NOTHING for me but made me feel like I’d been hit by a truck??
My dr said ‘maybe you’re just tough’ but now I know it’s genetics 😭
Also I uploaded my 23andme to GeneSight and it flagged 7 meds I’m on as risky. I’m going to my appt tomorrow with printouts. Wish me luck!!
PS: if anyone else has done this, DM me - I need to know who else is surviving this system 😅
sagar patel
Most doctors don’t care. They get paid to prescribe not to investigate. The system rewards volume not precision. Your genes don’t matter if your doctor doesn’t read the report.
Bailey Adkison
You people are so obsessed with genes it’s ridiculous. I’ve been on the same meds for 15 years. Never tested. Never had a problem. Your fear of biology is just a new form of medical anxiety.
Stop turning every side effect into a genetic crisis. Sometimes you just have a sensitive stomach. Sometimes you’re just unlucky. Not everything needs a DNA test.
Mussin Machhour
This is why I love community medicine. My grandma took statins for years, got muscle pain, stopped cold turkey - then got a heart attack. We didn’t know she had SLCO1B1 variant.
But here’s the thing - we fixed it. We found a doctor who listened. We got her tested. Switched to ezetimibe. She’s hiking again at 82.
It’s not about being perfect. It’s about being curious. Ask. Track. Share. You don’t need a PhD to be your own advocate.
And if your doctor rolls their eyes? Find a new one. Your life’s worth more than their convenience.
Zabihullah Saleh
There’s a quiet tragedy here. We’ve turned the human body into a machine that needs calibration - and we treat people like broken units instead of complex beings shaped by culture, stress, diet, sleep, trauma, and history.
Genes explain a lot. But they don’t explain why someone in rural Bihar responds differently to the same drug than someone in Brooklyn - even with identical SNPs.
Maybe the real frontier isn’t just pharmacogenomics.
It’s pharmacosociology.
What does it mean to heal a person when the system only sees a genome?