What Medicare Part D Formularies Actually Cover
Medicare Part D doesn’t just cover any drug you need. It covers only what’s on your plan’s formulary - a list of approved medications. And here’s the key: 92% of all prescriptions filled under Part D are generics. That’s not a coincidence. The system is built to push you toward cheaper, equally effective versions of brand-name drugs.
Generic drugs are chemically identical to their brand-name counterparts. They work the same way. They’re just cheaper because they don’t carry the cost of research, marketing, or patents. Part D plans make money by steering you toward these lower-cost options. And you save money too - if you know how the system works.
The Five-Tier System: Where Generics Live
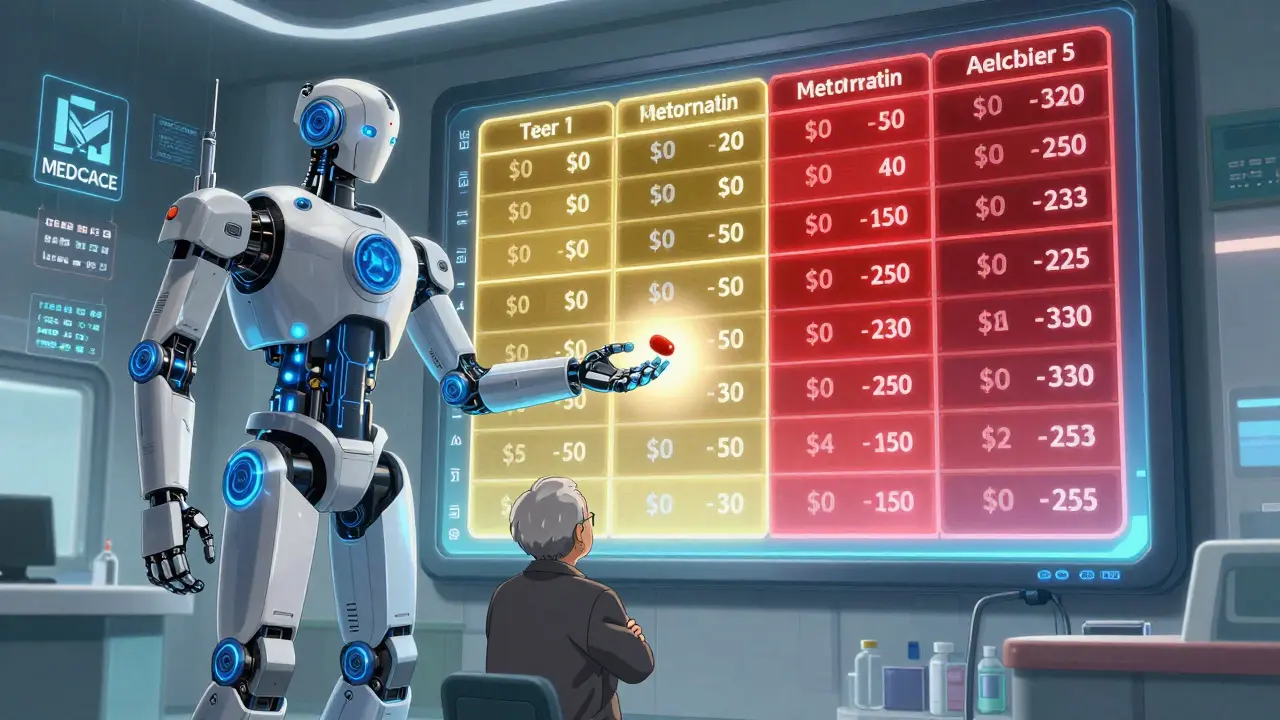
Every Part D plan puts drugs into five tiers. Think of it like a pricing ladder. The lower the tier, the less you pay.
- Tier 1: Preferred Generics - These are your best deal. Copays are usually $0 to $15 for a 30-day supply. Most common medications like lisinopril, metformin, or atorvastatin fall here.
- Tier 2: Non-Preferred Generics - Still generics, but not the plan’s top pick. You might pay $15-$40 or 25-35% coinsurance. This tier often includes newer generics or ones with less competition.
- Tier 3: Preferred Brand-Name Drugs - Brand-name drugs your plan encourages. You’ll pay more than generics, usually $40-$80.
- Tier 4: Non-Preferred Brand-Name Drugs - These are expensive. Copays can hit $100 or more. Often, you’ll need prior authorization to get them covered.
- Tier 5: Specialty Drugs - High-cost medications for complex conditions. These can cost hundreds or even thousands. Some plans put certain generics here too - especially newer ones for conditions like rheumatoid arthritis or hepatitis C.
Generics dominate Tiers 1 and 2. That’s intentional. Plans want you to pick the cheapest option. If your doctor prescribes a Tier 2 generic, you can often ask for a switch to a Tier 1 version. Many times, they’ll agree.
How Much You Pay in 2026
As of January 1, 2026, the rules changed again. The biggest change? You now pay a maximum of $2,100 out of pocket for all your drugs in a year - including generics.
Here’s how it breaks down:
- Deductible: You pay the first $615 of drug costs in 2025 (it’s $630 in 2026). Not all plans have a deductible - about half of them don’t. Check your plan’s details.
- Initial Coverage Phase: After you meet the deductible, you pay 25% of the cost for generics. Your plan pays the other 75%. This continues until your total out-of-pocket spending hits $2,100.
- Catastrophic Coverage: Once you hit $2,100, you pay nothing for the rest of the year. Not $0. Not $5. Not $10. Zero. For any drug - brand or generic.
That’s huge. Before 2025, people hit a coverage gap called the “donut hole.” You paid way more in that gap. Now, it’s gone. The cap means if you take three or four generics daily, you’ll likely hit the cap by late summer - and then your meds are free for the rest of the year.

Why Some Generics Aren’t Covered - Even If They’re the Same
Here’s where people get tripped up. Just because a generic exists doesn’t mean your plan covers it.
Example: Your doctor prescribes a generic version of losartan (a blood pressure drug). But your plan only covers valsartan - another drug in the same class. They’re both angiotensin II receptor blockers. They work similarly. But your plan doesn’t list losartan. So you pay full price unless you get an exception.
Plans do this to control costs. They pick one or two generics per class and encourage you to stick with them. If your preferred generic isn’t covered, you can file a coverage determination. In 2023, 83% of these requests were approved. You just have to ask.
Also, some plans don’t cover “authorized generics” - brand-name drugs sold under a generic label by the same company. They’re confusing because they look and cost like generics, but aren’t listed on the formulary. Always check the drug name exactly as it appears on your prescription.
How to Save Big on Generics
Knowing the rules isn’t enough. You need to act.
- Use the Medicare Plan Finder: Go to medicare.gov and enter your exact medications. Sort by lowest total cost. Don’t just pick the cheapest monthly premium. A $10 plan with high copays on your meds could cost you $1,200 more a year than a $40 plan with $0 generics.
- Check your Annual Notice of Change (ANOC): Every fall, your plan mails you a letter. It tells you if your drugs are moving tiers, getting removed, or if copays are changing. If your favorite generic is now Tier 3, it’s time to switch plans.
- Ask for a therapeutic interchange: Tell your pharmacist or doctor: “Is there a Tier 1 generic that works the same?” Often, they’ll switch it without you even needing a new prescription.
- Choose a $0 deductible plan: If you take multiple generics, a plan with no deductible saves you money from Day 1. 52% of stand-alone Part D plans offer this in 2026.
- Use mail-order pharmacies: Many plans give you a discount if you get a 90-day supply by mail. That cuts your copay in half.
Who Benefits the Most?
People on multiple generics win big. If you take three or more daily - say, metformin, lisinopril, and atorvastatin - you’re likely to hit the $2,100 cap by July or August. After that, your meds are free. That’s a $1,500+ annual savings.
Fixed-income seniors benefit most. Before the cap, a $40 copay on three generics added up to $1,440 a year. Now, if you hit the cap, that $1,440 disappears. And you’re not paying anything for the rest of the year.
But there’s a catch: confusion. A 2024 survey found that 62% of people taking generics understood their tier system. Only 42% of brand-name users did. If you don’t know your tiers, you’ll overpay.
What’s Coming Next
By 2026, every Part D plan must include a generic price comparison tool in their online member portal. You’ll be able to see which generic version of your drug costs the least - even across different brands.
In 2029, the government will start negotiating prices for certain generics. Insulin glargine (a common generic) is already on the list. That could bring prices down even further.
And by 2027, 95% of beneficiaries will have access to $0 copays for at least half of their commonly used generics. That’s up from 78% today.
Final Tips
Don’t assume your plan stays the same. Every year, 37% of plans change at least one generic’s tier. If you’re taking the same meds year after year, you’re vulnerable to surprise cost hikes.
Always double-check your formulary before enrollment. Use the Medicare Plan Finder. Don’t trust memory. Don’t trust your neighbor’s plan. Your drugs matter more than anything else.
If a generic isn’t covered, ask for an exception. You have a right to it. And if you’re spending over $2,100 a year on meds, you’re doing something wrong. The system is designed to cap you. Use it.
Frequently Asked Questions
Are generic drugs as effective as brand-name drugs under Medicare Part D?
Yes. Generic drugs contain the same active ingredients, work the same way, and meet the same FDA safety and effectiveness standards as brand-name drugs. The only differences are in inactive ingredients like fillers or coatings, which don’t affect how the drug works. Medicare Part D plans rely on generics because they’re proven to be just as effective - and far cheaper.
Why is my generic drug not covered even though it’s available?
Plans choose which generics to cover based on cost and agreements with manufacturers. Even if a generic exists, your plan might only cover one version in a drug class to keep prices low. If your prescribed generic isn’t on the formulary, you can request a coverage exception. In 2023, 83% of these requests were approved.
How does the $2,100 out-of-pocket cap work with generics?
The $2,100 cap (in 2026) includes only what you pay out of pocket for all drugs - including generics. Once you hit that amount, you pay $0 for the rest of the year. For generics, only your actual payment counts toward the cap. That’s different from brand-name drugs, where manufacturer discounts also count. This makes hitting the cap faster when you take mostly generics.
Can I switch plans if my generic gets moved to a higher tier?
Yes. Each fall, during the Annual Enrollment Period (October 15-December 7), you can switch to a different Part D plan. If your plan moves a generic to a higher tier or removes it entirely, use the Medicare Plan Finder to compare plans that cover your drugs at lower costs. You’re not stuck.
What should I do if my pharmacist gives me a different generic than I’m used to?
Pharmacists can substitute a different generic if it’s on your plan’s formulary - even if it’s not the one your doctor prescribed. If you’re charged more or your doctor didn’t approve the switch, ask the pharmacist to check your formulary. You can also call your plan to confirm coverage. If you’re unhappy, you can request a one-time refill of your original generic.



12 Comments
Ashley Porter
Just hit my $2,100 cap in July. Now my lisinopril and metformin are free. Feels like winning the lottery when you’re on a fixed income.
Peter Sharplin
Biggest mistake people make? Assuming their plan stays the same. I had a Tier 1 generic move to Tier 3 last year - didn’t notice until my copay jumped from $5 to $42. Caught it during ANOC review, switched plans, saved $900. Medicare Plan Finder is your best friend. Don’t wait till you’re overcharged.
Kipper Pickens
Therapeutic interchange is the unsung hero of Part D. Pharmacist asked if I wanted to switch from generic losartan to generic valsartan - same class, same efficacy, different formulary tier. I said yes. Copay dropped from $38 to $0. It’s not cheating, it’s optimization. The system’s designed for this. Use it.
Also, authorized generics? Don’t get fooled. That’s just the brand selling the same pill under a different label. Not on formulary = not covered. Always check the NDC code, not just the name.
And yes, the $2,100 cap includes all out-of-pocket spending - but only your payments count for generics. Manufacturer discounts don’t apply. That’s why folks on multiple generics hit the cap faster. It’s not a bug, it’s a feature.
If you’re paying more than $150/month for generics and you’re not on a $0 deductible plan, you’re doing it wrong. 52% of plans offer no deductible. Find one. Seriously.
And stop trusting your neighbor’s plan. My sister’s on the same plan as me - she takes two drugs I don’t. Her ‘cheap’ plan is my financial nightmare. Every year, I re-enroll. Every year, I compare. It’s not optional anymore.
Also, mail-order 90-day fills? If your plan offers it, use it. Half the copay. Same meds. No extra effort. I’ve been doing it for three years. Saved $480 last year alone.
And yes, you can file for a coverage exception. 83% approval rate. You don’t need a PhD in pharmacology. Just write a letter. ‘My doctor prescribed X, it’s clinically equivalent to Y on formulary, and I’ve been stable on it for 18 months.’ Done. Approved.
They want you to use generics. They just want you to use the *right* ones. Know your tiers. Know your formulary. Know your rights.
Joanna Domżalska
Wow. So the government capped drug costs so seniors don’t go broke… but only if they take generics. What if you have a rare autoimmune disease and need a brand-name biologic? You’re screwed. This isn’t healthcare reform. It’s generic promotion with a side of virtue signaling.
shivam utkresth
Bro, the way you’re talking about generics like they’re some secret hack - it’s just common sense. I’m from India, we’ve been using generics since the 80s. Same molecule, same results, 1/10th the price. Why is this news here? Also, ‘authorized generic’? That’s just the brand playing both sides. Like McDonald’s selling a ‘homemade burger’ with their own beef. Stop being surprised by capitalism.
But hey, at least now you’ve got a cap. We don’t even have that. My cousin in Delhi pays $200/month for insulin. No cap. No plan. Just hope.
So yeah, use the Plan Finder. Switch if needed. Ask for the interchange. But don’t act like this is some revolutionary insight. It’s just basic math. And maybe, just maybe, the system’s finally catching up to the rest of the world.
John Wippler
For real - if you’re taking three or more generics daily, you’re basically getting paid to be healthy. Hit the cap by August? Your meds are free. That’s not a policy. That’s a gift. And yet people still don’t check their ANOC. They just keep paying the same copay like it’s magic.
I tell my elderly aunt every year: ‘Don’t just sit there. Look it up. Call your pharmacist. Ask for the Tier 1 version.’ She did last fall. Switched from a $25 generic to a $0 one. Now she laughs when she sees her bill. ‘I’m getting paid to take my pills,’ she says.
This system works. But you gotta be the CEO of your own health. No one else will do it for you.
rasna saha
Thank you for explaining this so clearly. I’ve been scared to switch plans because I didn’t understand the tiers. Now I feel like I can actually take control. I’m going to check my meds on Medicare.gov tonight. You made this feel doable.
Aurelie L.
So now you’re not allowed to pay more than $2,100… but your doctor still charges $120 for a 10-minute visit to adjust your meds. Who’s really saving here?
James Nicoll
So the government finally figured out that if you make generics cheaper, people will take them. Groundbreaking. Next they’ll tell us water is wet and oxygen is breathable. Meanwhile, the pharmaceutical industry just shifted their profits from brand-name patents to formulary exclusivity deals. Same scam, new packaging.
And don’t get me started on ‘therapeutic interchange.’ That’s just pharmacy automation pretending to be patient care. ‘Oh, we switched your blood pressure med to a different one - no need to see your doctor, we’ve got the algorithm.’
But hey, at least your pills are free after August. That’s something. I guess.
Faisal Mohamed
It’s not about generics. It’s about control. The system doesn’t care if you’re healthy. It cares if you’re predictable. Generics are the perfect compliance tool - cheap, standardized, easy to track. We’re not being helped. We’re being optimized.
And yet… here I am, paying $0 for my statin after August. So maybe the machine, in its cold, bureaucratic wisdom, has accidentally created a small corner of compassion.
🫡
Uche Okoro
Formulary design is a classic example of cost-shifting disguised as consumer empowerment. The plan’s incentive structure is engineered to minimize aggregate expenditure, not maximize individual health outcomes. The $2,100 cap is a fiscal artifact of the Inflation Reduction Act’s political calculus - not a medical advancement. The real innovation is the algorithmic prioritization of therapeutic equivalence over clinical nuance. Patients are treated as data points, not persons. And yet, paradoxically, the system’s efficiency has produced an unintended welfare gain for the most pharmacologically dependent. The irony is not lost on those who understand the structural contradictions of neoliberal healthcare.
John Wippler
And that’s why you don’t just sit back and wait for the system to fix you. You get on the phone. You call your doctor. You ask for the Tier 1 version. You use mail-order. You check your ANOC. You switch plans. You file for exceptions. You don’t just ‘hope’ it works. You make it work. Because if you don’t, no one will. And yeah - it’s a lot of work. But when your meds are free for six months? It’s worth every minute.